We see increasing excitement about Medicare’s new Advanced Primary Care Management (APCM) program. Done well, APCM could be transformative for primary care practices and their patients. APCM provides fee-for-service reimbursement for providers to deliver high-value, proactive care across entire populations. APCM will be a financial lifeline for physicians, enabling them to invest in staffing and services that will directly benefit patients.
But to see those benefits, you have to do APCM well.
A poorly-executed APCM launch will disrupt your operations and destabilize your finances. Worst of all, low-quality APCM will diminish the trust your patients have in your practice. You must have a thoughtful, comprehensive plan for your APCM program.
Care management contributes to better health outcomes and reduces the total cost of care (TCoC), two primary goals for CMS. APCM is a fee-for-service reimbursement program that creates incentives for providers to move toward value-based care.
Both Chronic Care Management (CCM) and APCM are intended to drive value-based outcomes, but APCM is generally better for primary care providers.

WEBINAR
To learn more about APCM and CCM, watch our on-demand webinar. This comprehensive comparison will help you evaluate which program is the best fit for your practice.
If you want your APCM program to achieve long-term financial sustainability, consider 5 key elements of your plan:
Here are some questions you should think through. (Ideally, do this before you begin enrollment and patient consent!)
A successful APCM program will create value for all stakeholders:
In my last article, I explained that APCM success hinges on creating value for your patients. Many patients will have a cost sharing responsibility. To retain patients in APCM, your practice must deliver excellent care management at scale.
But high-quality care management is just one of the pillars that drives APCM program success and financial sustainability.
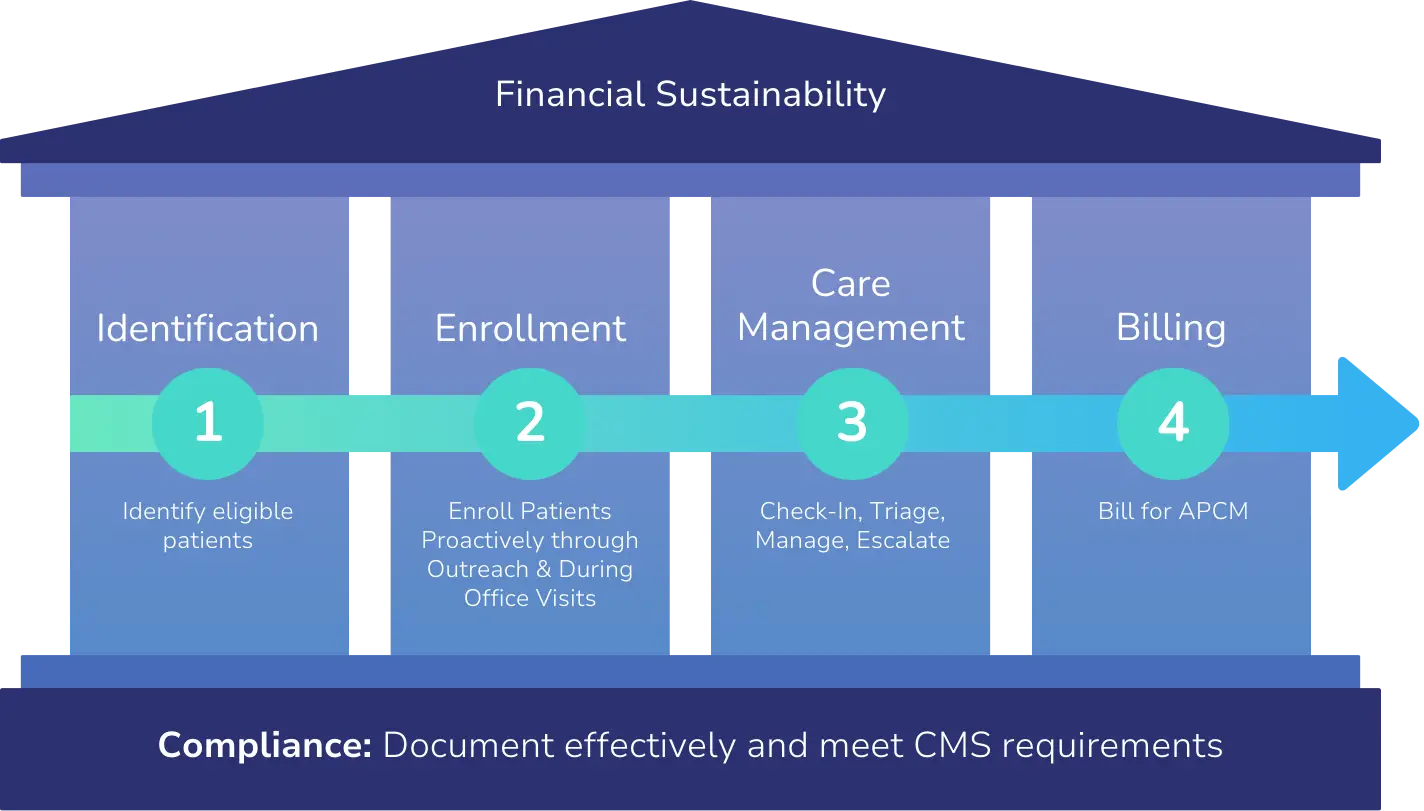
Here are descriptions of each pillar, and some key questions you should ask as you develop your APCM plan.
Currently, patients enrolled in Traditional Medicare are eligible for APCM. We expect Medicare Advantage plans will eventually reimburse practices for APCM. However, reimbursement may vary considerably compared to Traditional Medicare.
(For CCM, Traditional Medicare reimburses at $62.58 for 20 minutes of care. But Medicare Advantage plans reimburse anywhere from $0 or $2 up to $80 for that same 20 minutes. APCM reimbursement will likely show similar variation.)
As you think about identifying eligible patients, consider the following questions:
This will help you understand potential utilization and reimbursement. It will also help you understand the cost-sharing burden for patients. Finally, planning ahead for Medicare Advantage reimbursement will help you expand your program in the future.
Patient enrollment is more complex than you might think! Medicare seems to expect every patient to be enrolled, which sounds great:
“We anticipate that a practitioner using the advanced primary care model will bill for APCM services for all or nearly all the patients for whom they intend to assume responsibility for primary care.”
But it’s not that easy. You will need a strategy, plan, and tools to manage enrollment.
You can enroll patients during an initiating visit, such as an annual wellness visit. However, Medicare rules give you the flexibility to enroll existing patients proactively through outreach:
“An initiating visit is not needed: (1) if the beneficiary is not a new patient (has been seen by the practitioner or another practitioner in the same practice within the past three years) or (2) if the beneficiary received another care management service (APCM, CCM, or PCM) within the previous year with the practitioner or another practitioner in the same practice.”
(Note that participating in the ACO REACH Model, the Making Care Primary model, or the Primary Care First model will satisfy the initiating visit requirement for assigned beneficiaries.)
Consider how you will educate patients during the enrollment process:
Again: “Enroll and bill for every patient” may sound great. But it’s not that easy.
High-quality care management is the essence of APCM. Good care drives outcomes and creates value for patients – critical when many patients will have cost-sharing responsibility.
Consider how you might scale quality care:
Consider how you will integrate APCM services with the rest of the work your organization does:
Remember, many patients will have cost-sharing. They have to believe the program is “worth it” – month in and month out. Consider how you will deliver and demonstrate value to your patients:
WIth APCM, CMS is pushing you to think about the care management needs of your patient population as a whole.
Consider how you will achieve the population health management goals built into APCM:
Smart billing ensures financial sustainability for your program. You may be familiar with time-based reimbursement for CCM. APCM reimbursement is different.
APCM reimbursement is not time-based, so you could bill for every consented patient, every month. Reimbursement depends on the number of chronic conditions and Qualified Medicare Beneficiary (QMB) status.
| Code | Patient Population | % of Patients | Est. Monthly Reimbursement (Per Patient) | Est. Annual Reimbursement (Per Patient) |
|---|---|---|---|---|
|
G0556 |
≤1 Chronic Condition |
~20% |
$15 |
$180 |
|
G0557 |
2+ Chronic Conditions |
~70% |
$50 |
$600 |
|
G0558 |
2+ Chronic Conditions & QMB Status |
~10% |
$110 |
$1,320 |
There’s a lot to think about here.
Phamily is the market leader in high-quality, large-scale proactive care management. We’re happy to help you think through these questions – and many others – in more detail.
We can also provide a customized pro forma that synthesizes all the complex operational, clinical, and financial considerations your practice must evaluate.

Darshan has 15+ years experience co-founding and building high growth healthcare technology businesses committed to improving access to care and quality of care. More about Darshan…